Infection Control Checklist for Shared Living Spaces [2026 CDC Guidelines]

Shared living facilities, like nursing homes and group homes, face constant infection risks due to shared spaces and vulnerable populations. The CDC's 2026 guidelines focus on managing respiratory viruses like influenza, RSV, and SARS-CoV-2 through tailored, risk-based strategies. Key measures include isolating symptomatic residents, enhancing cleaning protocols, enforcing PPE use, and improving ventilation. These steps help protect residents and staff while maintaining dignity and care quality.
Key Updates:
- Isolate symptomatic residents in single rooms when possible.
- Use EPA-approved disinfectants for high-touch surfaces.
- Enforce N95 respirators and strict hand hygiene for caregivers.
- Track outbreaks with detailed logs and rapid testing schedules.
Effective infection control ensures safety and reduces the spread of illnesses in shared living spaces.
Infection Prevention and Control in the Care Home
sbb-itb-45288fe
Daily Resident Management Checklist
Managing residents effectively on a daily basis starts with quickly identifying and isolating those showing symptoms. According to updated CDC guidelines, residents with respiratory symptoms should be placed in single-person rooms with dedicated bathrooms. If this isn't possible, exposed roommates must follow strict source control measures to reduce transmission while preserving their dignity and social interactions. Below are actionable steps to help minimize infection risks for both residents and staff.
Isolating Residents with Symptoms
When a resident shows symptoms, they should be placed in a single-person room with a dedicated bathroom. If this isn't an option, apply strict Transmission-Based Precautions, including improved ventilation and air filtration. Healthcare personnel entering these rooms must wear NIOSH-approved N95 respirators, gowns, gloves, and eye protection.
It's worth noting that over 40% of older adults with influenza may not experience a fever of 100.4°F. Look for less obvious signs like behavioral changes, dizziness, or nausea, which may indicate an infection before respiratory symptoms develop. Starting antiviral treatments for influenza within 48 hours of symptom onset can significantly improve outcomes.
Residents under Transmission-Based Precautions should stay in their rooms unless leaving for essential medical purposes. This restriction is crucial during the virus's incubation period, which usually lasts 12 hours to 5 days but can extend to 8 or even 14 days for some variants.
Managing Roommates and Visitors
Roommates of symptomatic residents are considered exposed and must wear facemasks around others to prevent spreading the infection. Avoid moving exposed roommates into rooms with unexposed residents to limit further risks.
Screen all visitors using no-touch infrared thermometers and symptom checklists. Visitors with a temperature of 100.4°F or higher or respiratory symptoms should delay their visits. During outbreaks, the CDC advises that indoor visits take place only in the resident's room:
"If indoor visitation occurs [during an outbreak], visits should ideally occur in the resident's room, and visitors should not linger in other areas of the facility or engage with other residents."
Maintain a centralized log of visitor details to streamline contact tracing if needed. Visitors showing respiratory symptoms should postpone non-urgent visits until they're no longer contagious.
Restricting Movement for Sick Residents
Residents with symptoms should only leave their rooms for medically necessary activities. When they do, they must wear facemasks and maintain physical distance from others.
To prevent cross-contamination, assign dedicated medical equipment - such as blood pressure cuffs, thermometers, and pulse oximeters - for use only with symptomatic residents. For bedding, consider using PeelAways disposable sheets. These allow staff to quickly remove soiled layers, revealing a clean and waterproof sheet underneath, which can be replaced in just 60 seconds.
To support residents' emotional and social needs during restricted in-person visits, encourage the use of video-call applications. As emphasized by the UK Health Security Agency:
"proportionate, risk-based and time limited interventions are required to protect health, social and emotional wellbeing of residents".
Finally, establish clear exit criteria with defined clinical benchmarks to determine when a resident can safely end isolation and rejoin communal activities. These steps, combined with infection control strategies in shared living spaces, help maintain a balance between infection control and resident well-being.
Cleaning and Hygiene Routines Checklist
Keeping shared living spaces clean and disinfected is essential for controlling infections. According to the CDC, this means having daily cleaning routines for occupied rooms and more thorough terminal cleaning when residents leave or transfer. Special care is needed for high-touch surfaces, bedding, and shared bathrooms. Using EPA-approved disinfectants is key to removing pathogens and stopping cross-contamination. Below are some core cleaning and hygiene practices to follow.
Disinfecting High-Touch Surfaces
High-touch surfaces are hotspots for germs and need frequent disinfection throughout the day. Focus on areas like doorknobs, light switches, handrails, elevator buttons, faucet handles, and toilet flush levers. These should be cleaned multiple times daily with EPA-approved disinfectants. Always work in a "clean to dirty" direction to avoid spreading germs to clean areas.
Save floor cleaning for last to avoid re-contaminating surfaces. For blood or body fluid spills, immediately absorb the liquid with designated pads, then disinfect the area with an intermediate-level disinfectant.
Remember, cleaning removes dirt, sanitizing lowers germ levels to safer amounts, but disinfection is what truly eliminates pathogens. For shared living spaces, disinfection is the gold standard for high-touch surfaces.
Bedding and Linen Management
Bedding needs regular care - both during daily room cleaning and with terminal cleaning when residents leave or transfer.
Products like PeelAways multi-layer disposable sheets make this process faster. Staff can peel away a soiled layer in just 60 seconds, revealing a fresh, waterproof sheet underneath. This method cuts laundry needs by 50-80% while maintaining hygiene standards.
The same thorough approach applies to communal bathrooms and public spaces.
Cleaning Bathrooms and Shared Spaces
Shared bathrooms should be cleaned and disinfected at least twice daily to prevent germ buildup. Pay close attention to faucets, handles, toilet seats, and door handles - these are high-touch areas that residents interact with before and after washing their hands.
Facilities should also set a Minimal Cleaning Time for different room types. This ensures staff have enough time to properly follow all disinfection steps without rushing, as hurried cleaning can compromise infection control. Room size and complexity should guide how much time is allocated for cleaning tasks.
Staff and Caregiver Protection Checklist
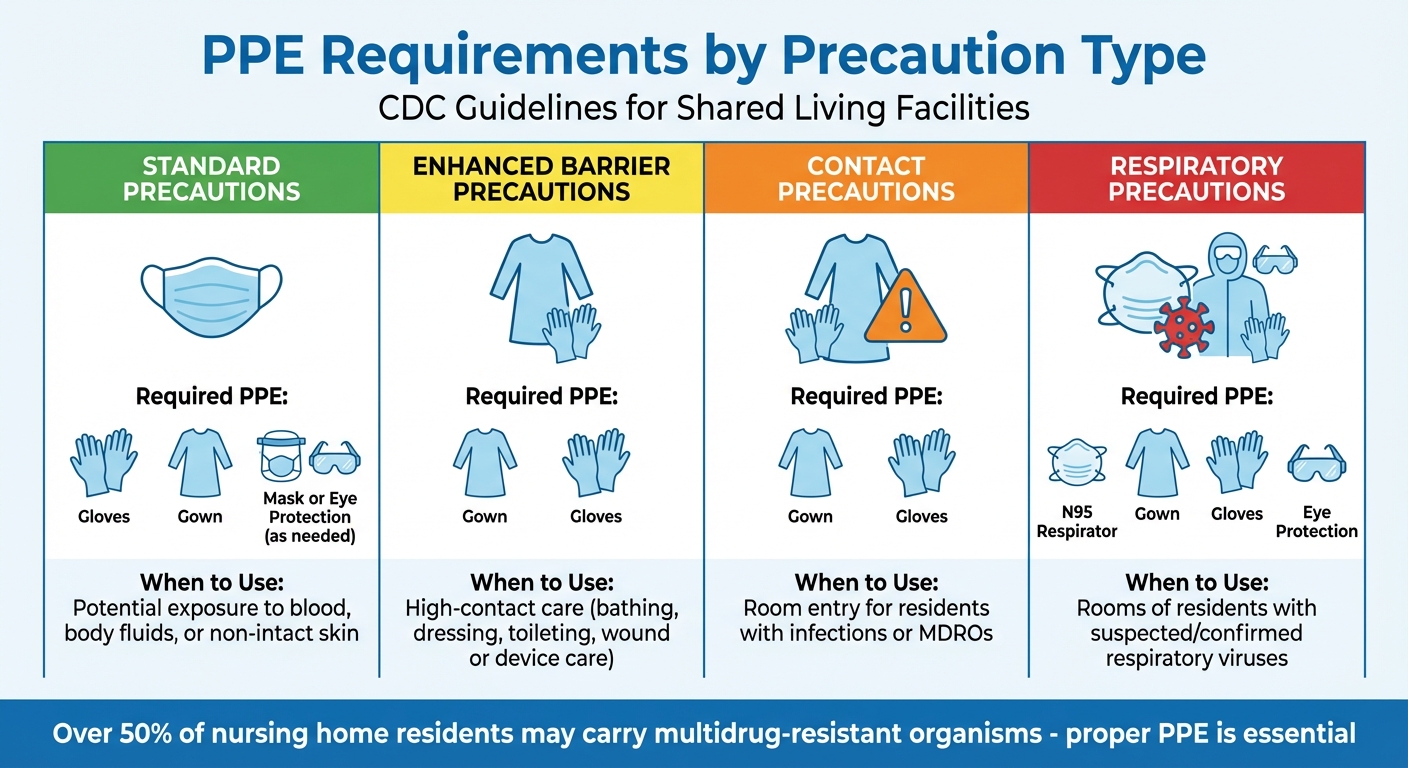
PPE Requirements by Precaution Type in Shared Living Facilities
Staff and caregivers play a crucial role in preventing infections by using personal protective equipment (PPE) properly, practicing strict hand hygiene, and guiding visitors on safety measures. According to CDC guidelines, over 50% of nursing home residents may carry multidrug-resistant organisms, underscoring the importance of these practices.
Using PPE and Protective Equipment
The type of PPE used should match the level of care provided and the infection risks associated with each resident:
- Standard Precautions: Use gloves, gowns, facemasks, or eye protection when there's potential contact with blood, body fluids, secretions, or non-intact skin.
- Enhanced Barrier Precautions: Require gowns and gloves during high-contact activities like bathing, dressing, transferring, toileting, changing linens, or managing medical devices.
- Contact Precautions: Residents with confirmed infections, such as those with acute diarrhea, draining wounds, or during MDRO outbreaks, require staff to wear gowns and gloves every time they enter the room.
- Respiratory Precautions: When respiratory viruses are suspected, staff should wear an N95 respirator along with a gown, gloves, and eye protection.
Facilities should clearly post precautionary signage outside resident rooms and place trash cans near room exits for safe disposal of used PPE.
| Precaution Type | Required PPE | Situation for Use |
|---|---|---|
| Standard | Gloves, gown, mask, or eye protection (as needed) | Potential exposure to blood, body fluids, or non-intact skin. |
| Enhanced Barrier | Gown and gloves | High-contact care (e.g., bathing, dressing, toileting, wound or device care). |
| Contact | Gown and gloves | Room entry for residents with infections or MDROs. |
| Respiratory | N95 respirator, gown, gloves, eye protection | Rooms of residents with suspected/confirmed respiratory viruses. |
PPE use should always be paired with rigorous hand hygiene protocols, which are covered in the next section.
Enforcing Hand Hygiene
Proper hand hygiene is essential to infection control. Staff should wash their hands with soap and water or use an alcohol-based sanitizer:
- Before and after every resident interaction
- After glove removal
- After touching potentially contaminated surfaces
During norovirus or gastrointestinal outbreaks, soap and water should be used instead of alcohol-based sanitizers, as these are less effective against norovirus.
Facilities can monitor compliance using methods like direct observation, fluorescent markers, or ATP assays. Regular training - conducted at hiring, annually, and whenever new protocols are introduced - helps reinforce these practices. Maintaining formal competency records ensures accountability. Since older adults in shared living environments may show unusual signs of infection, such as dizziness or behavioral changes, consistent hand hygiene is even more critical.
Educating Visitors on Hygiene
Visitor education is another key component of infection prevention. Facilities should provide easily understandable materials like handouts, posters, and graphics to emphasize infection prevention practices and the importance of staying current with immunizations. Visitors with respiratory symptoms or recent exposure to infections should delay non-urgent visits or wear masks during their time in the facility.
"Visitors should be counseled about their potential exposure to respiratory infection in the facility. If indoor visitation occurs, visits should ideally occur in the resident's room, and visitors should not linger in other areas of the facility or engage with other residents".
Residents can also play a role by encouraging their visitors to practice proper hand hygiene. Additionally, establishing protocols for storing visitor belongings can help maintain clear surfaces, making cleaning and disinfection more effective.
Outbreak Response and Monitoring Checklist
When dealing with an outbreak, it's crucial to act quickly and effectively. This means implementing rapid testing, improving ventilation, and keeping meticulous records. According to the CDC's 2026 guidelines, these steps are essential to control transmission and safeguard vulnerable groups. Building on earlier protocols for residents, cleaning, and staff, this section focuses on outbreak-specific measures.
Tracking Transmission and Testing
Testing plays a key role in managing outbreaks. Any resident or staff member showing even mild symptoms should be tested immediately, regardless of vaccination status. For those exposed but asymptomatic, follow a three-test schedule on Days 1, 3, and 5.
During active outbreaks, expand testing to include all residents and staff in affected areas. Repeat testing every 3–7 days until no new cases are detected for at least 14 days. For individuals who recovered from infection within the last 31–90 days, antigen tests are preferred, as NAAT tests may remain positive even after the person is no longer contagious.
Thorough documentation is equally important for identifying trends and reporting to health authorities. Maintain centralized logs that include daily screening results, contact tracing data, and outbreak metrics. Here's a quick reference for what to track:
| Tracking Category | Data Points to Document | Frequency |
|---|---|---|
| Daily Screening | Name, temperature (≥100.4°F), symptoms, time of entry | Every entry/Daily |
| Resident Health | Respiratory/GI symptoms, mental status changes, vaccination status | Twice daily (Outbreak) |
| Contact Tracing | Interaction logs, shared activities, staff assignments | Continuous |
| Outbreak Status | Symptom onset dates, hospitalizations, isolation status, test results | Daily updates |
Reports to health authorities should include resident demographics, symptom onset dates, potential exposure sources, and isolation details. Additionally, the CDC highlights the importance of wastewater surveillance systems to detect infectious threats early, even before clinical cases emerge.
Improving Ventilation
Air quality becomes a critical factor during outbreaks. Work with facility engineers to enhance ventilation in both private rooms and communal areas. Portable HEPA air purifiers can help in spaces with poor ventilation, while UV-C light systems in HVAC ducts can neutralize airborne pathogens.
When conditions allow, open windows and doors to increase natural airflow. Use CO2 monitors to assess air circulation - lower CO2 levels indicate better ventilation. During outbreaks, replace air filtration systems and clean ductwork more frequently than usual.
Humidity also plays a role in respiratory health. Aim to keep indoor humidity between 40% and 60%, using humidifiers or dehumidifiers as needed. To reduce aerosol concentration, limit the number of people in shared spaces by scheduling staggered activities. In poorly ventilated areas where residents cannot wear masks, staff should wear NIOSH-approved N95 respirators for added protection. These steps, combined with regular cleaning routines, help minimize airborne risks.
Ending Isolation for Recovering Residents
Clear guidelines for ending isolation are vital to protect both individuals and the broader community. For residents with mild to moderate illness, isolation can generally end after 10 days, provided they’ve been fever-free for 24 hours without medication and symptoms are improving. For severe cases, isolation may last up to 20 days.
Residents who are moderately to severely immunocompromised need a test-based approach to determine when isolation can end. This involves two negative viral tests (NAAT or antigen) taken 48 hours apart. Residents exposed to the virus who cannot be tested or wear masks should remain under Transmission-Based Precautions for 10 days after exposure.
Even after isolation ends, continue monitoring for symptom recurrence and maintain enhanced cleaning in their living areas. During periods of high transmission, basic source control measures should remain in place to ensure ongoing safety for everyone.
Conclusion
Protecting shared living spaces like nursing homes requires a multi-faceted approach that prioritizes vaccination, rapid testing, strict hygiene practices, and prompt isolation when necessary. The CDC underscores this by stating, "Preventing the spread of respiratory viruses in nursing homes requires a comprehensive approach that includes not only vaccination, but also testing, treatment, and the prompt implementation of proven infection prevention and control measures". By adhering to the 2026 guidelines, which cover everything from daily screenings to PPE protocols and outbreak monitoring, you can create effective barriers against transmission and safeguard at-risk populations.
The measures outlined in the checklists above not only reduce infection risks but also enhance care workflows. Proper PPE, improved ventilation systems, and diligent monitoring are essential components. Additionally, digital tools like SafetyCulture simplify compliance tracking, ensuring protocols are followed efficiently. Bedding management is another critical factor - using waterproof, disposable options eliminates the need for heavy mattress lifting, reduces caregiver strain, and minimizes cross-contamination. Products like PeelAways multi-layer disposable sheets allow for quick bedding changes, maintaining high hygiene standards while addressing workflow challenges and preserving residents' dignity.
These strategies go beyond improving safety - they can also lead to cost savings and operational efficiencies. For instance, PeelAways is offering blog readers an exclusive 10% discount on their multi-layer disposable sheets. Use code BLOGS10 at checkout to save. This discount can be combined with subscriptions and bundle offers, helping you save money while simplifying care routines.
You can purchase PeelAways products on Amazon or directly from Peelaways.com.
FAQs
What should we do if we don’t have enough single rooms for isolation?
If single rooms aren't an option, the 2026 CDC guidelines offer practical steps to lower transmission risks in shared spaces. Here's what to do:
- Prioritize hand hygiene: Regular and thorough handwashing is essential.
- Use PPE properly: Ensure personal protective equipment is worn correctly at all times.
- Clean shared spaces often: Frequently disinfect high-touch surfaces and communal areas.
- Dedicate equipment: Assign medical or personal equipment exclusively to infected individuals.
- Utilize privacy curtains: These can act as barriers to reduce contact between individuals.
- Maintain distance: Keep at least three feet of space between beds in shared rooms.
By sticking to these steps, you can help limit cross-contamination and reduce the spread of infections in shared living environments.
How often should we disinfect high-touch surfaces during an outbreak?
During an outbreak, it's important to disinfect high-touch surfaces regularly - ideally every day or even more often if needed. This simple step helps lower the risk of infection and ensures shared living spaces remain safer for everyone.
What’s the simplest way to track testing, symptoms, and visitor logs?
The easiest way to monitor testing, symptoms, and visitor activity in shared living spaces is by using organized logs or checklists. Tools like no-touch thermometers and symptom checklists make entry screenings straightforward and effective. Keeping a standardized log - whether on paper or digitally - for test results, symptoms, and visitor entries ensures accurate and consistent tracking. This approach aligns with the 2026 CDC guidelines for managing infection control in shared environments.
Comments
0



SAVE MONEY & WATER
Professionals & Institutions save a fortune on labor/laundry.

SUPERIOR COMFORT
The first thing our customers notice is how soft our sheets are.
100% WATERPROOF
Each layer is 100% Waterproof, perfect for spills and accidents

SAVE TIME
Change the sheet in under 1 minute without stripping the bed.
Leave a comment